If you are anything like us you might have spent the last few months shedding tears over episodes of ‘This Is Us’. And, if you haven’t had a chance to check out this awesome series sorry in advance for a tiny spoiler alert. Also, start watching immediately after you read this!
Now, as if we didn’t love the show enough, they introduced a pregnancy storyline with Kate, one of the central characters. If there is one thing we love more than binge-watching shows that leave us crying into our popcorn, it’s pregnancy and birth.
Coincidentally, we have also spent the last few months on what we’ve called a #bopo (body positivity) podcast circuit where we were able to bust common plus-size birth myths, which we absolutely loved doing.
This discussion is important for many reasons. Not only do over 50% of women (1) fall into the category of overweight or obese (yes we hate that word too!), they are likely to face discrimination and fat-shaming language by both society and their health care providers during their pregnancy and birth.
For proof of this, you don’t need to look much further than the scads of articles posted after Kate’s pregnancy announcement on the show, deeming her pregnancy high-risk at just 6 weeks, long before any diagnostic testing.
So, does a plus size body automatically equal a high-risk pregnancy and highly medicalized birth?
This is a tough question to answer for many reasons; one of the reasons being that the scale by which we measure obesity is deeply flawed, along with the assumption that all women who are plus size are unhealthy.
The standard tool for determining your body mass index is the BMI scale:
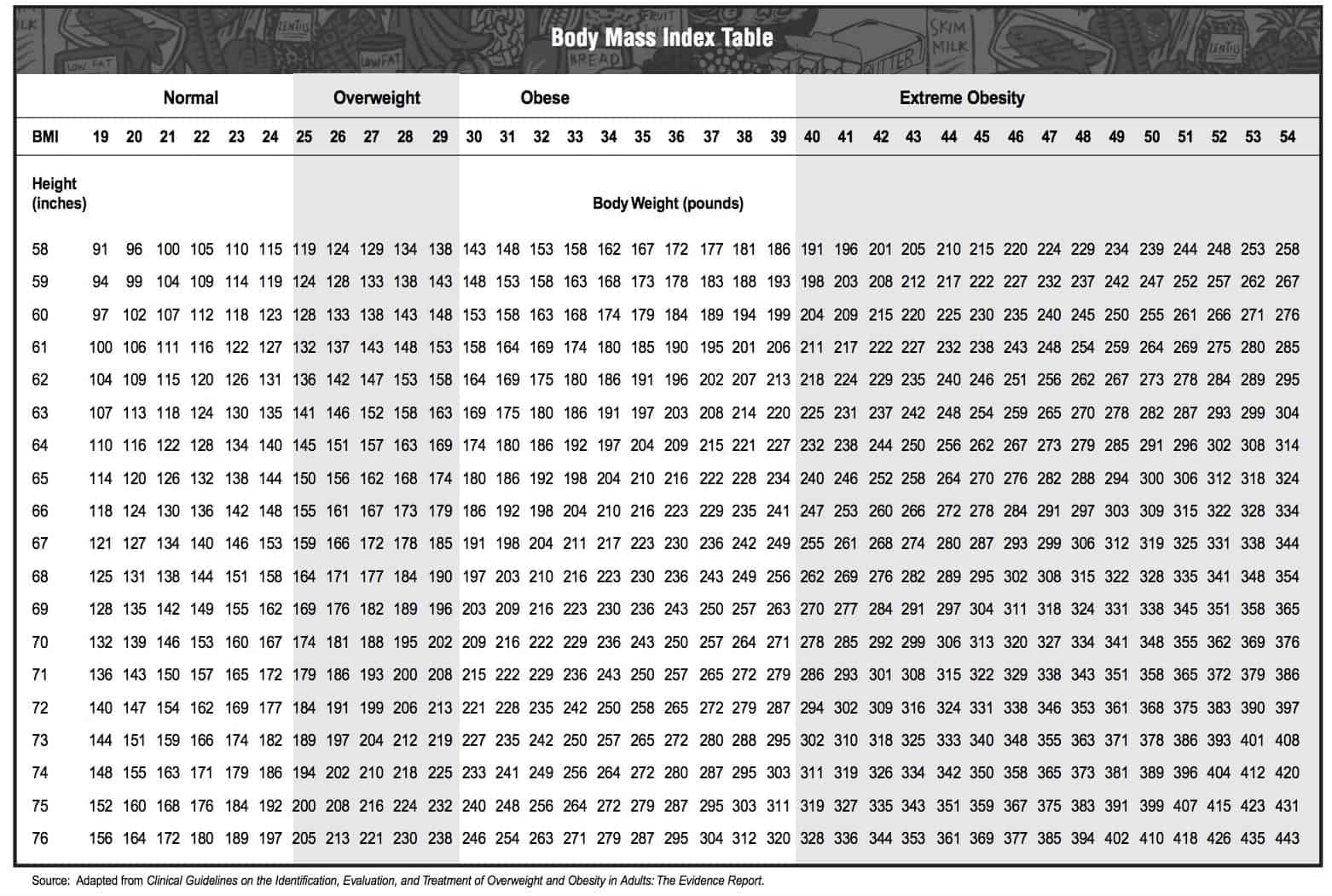
As you can see, this chart is simply taking into account the height and weight of an individual, not the fitness level, lifestyle, age, economic status, ethnicity or health history.
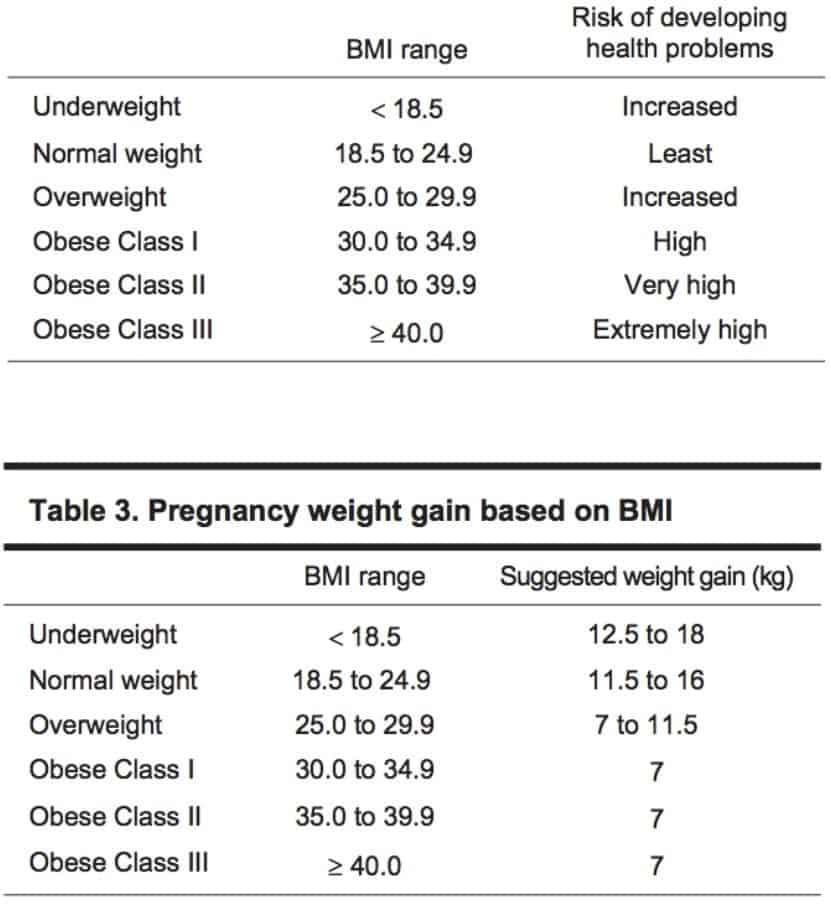
For these reasons, a BMI of ≥ 30 alone does not necessarily mean a high-risk pregnancy. Compounding factors such as the list above, as well as pre-existing and/or concurrent health conditions must be taken into account. Most women who wear plus size clothing will go on to have a healthy pregnancy and positive birth.
What Are the Risks?
It is no secret that a plus size pregnancy does come with elevated risks such as gestational diabetes, hypertension, and preeclampsia. And these risks increase as the BMI increases. One study showed an increase in Gestational Diabetes from 6.74% in the overweight category to 13.42% in the Obese Class 1 (see chart below) category (2). What is important to note with these numbers, is that in spite of what many think, including some health care providers, a BMI of >30 does not automatically mean you will test positive for complications.
In fact, these complications can be present for women of all sizes, including those in the ‘normal weight’ range and there is much that can be done in pregnancy to reduce these risks. For example, there is a 34% reduction of Gestational Diabetes with brisk walks 3 or 4 times a week (3). Even if a person starts a pregnancy with a higher BMI, the outcomes are more ideal when they stick to the recommended weight gain listed in this chart:
This does not mean crash dieting and food restricting to stay within a certain range. Instead, it means encouraging positive changes such as eating more whole foods, reducing processed foods and adding exercises such as walking and prenatal specific yoga. Taking care of your amazing plus size body during pregnancy yields outcomes that are closer to those of someone with a ‘normal’ BMI. (4)
Big Babies & Cesarean Birth
One thing we continually hear is that women who are considered plus size are more likely to birth big babies and we have been conditioned to believe that having a big baby is scary. We highly recommend reading the article ‘Evidence On: Induction or Cesarean for a Big Baby’ if you feel like you are in this category.
The medical term for ‘big baby’ is macrosomia (baby weighing more than 4000g) and while macrosomia is more common in individuals with a BMI of ≥ 30, it is more common with those who have Gestational or Type 1 or 2 Diabetes. Even still, managing diabetes with diet, exercise, staying within the recommended weight gain guidelines, and/or medication brings the risk back down to normal levels (5)(6). Staying within recommended weight gain guidelines also reduces the risk of macrosomia (7).
Image courtesy of Evidence Based Birth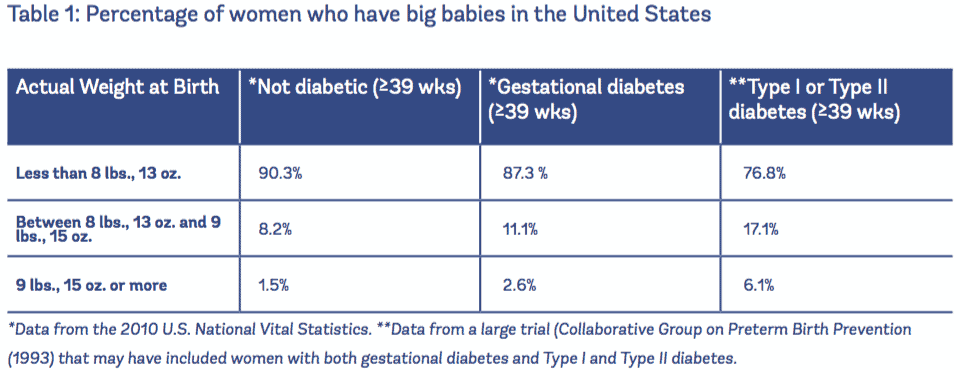
A worry that many of us have around big babies is shoulder dystocia, and although macrosomia is a risk factor for shoulder dystocia, the absolute risk of shoulder dystocia remains low (8). Plus size women may be told that as they are at risk for a larger baby, their baby is at risk for getting stuck and a cesarean birth is recommended. Before we explain even further what could be wrong with that statement, we want to note in a study where patients with hypertension and diabetes were removed, there was no increased risk for shoulder dystocia in the obese population. Maternal obesity is not an independent risk for shoulder dystocia (9).
One of the real problems here is that ultrasounds for a suspected big baby are flawed and often associated with interventions such as induction and cesarean section (10). One study showed that of 86 women whose babies were estimated at larger than 4000g, 77% of ultrasounds were incorrect, estimating higher than the actual birth weight (10).
According to the ACOG, suspected fetal macrosomia is not an indication for delivery and rarely is an indication for cesarean delivery with a recommendation that cesarean delivery be limited to estimated fetal weights of at least 5,000 g in women without diabetes and at least 4,500 g in women with diabetes (11).
The next problem we face is that a cesarean birth is not ideal for women with a BMI above the ‘normal’ range and puts them at risk for complications such as infection (12), thrombosis (13), and postpartum hemorrhage (14). Neither the SOGC or the AOM identify a BMI of ⪰30 alone as an indication for a cesarean section. Instead, recommendations include careful monitoring of other risk factors, as mentioned above, as well as encouraging good nutrition and exercise to reduce these risk factors.
Longer labours
Another common reason women are told that a cesarean birth might be necessary is ‘failure to progress’; a common reason for cesarean births that we hear for all body sizes.
While studies do show that a higher BMI is linked to a longer labour, the increase is small, however, the evidence does show that labour times increase as BMI increases. One study shows a duration of 6.2 hours for a ‘normal’ weight compared to 7.9 hours from 6cm to 10cm dilation for obese women (15). Interestingly, in this study, there were no difference in the second (pushing) stage of labour.
Another, more recent study showed a slower progression during early labour, particularly between 4cm and 6cm dilation, picking up after 6cm showing relatively similar progress between normal weight and obese women (16). Below is a chart from this study showing the labour curve by body mass index.
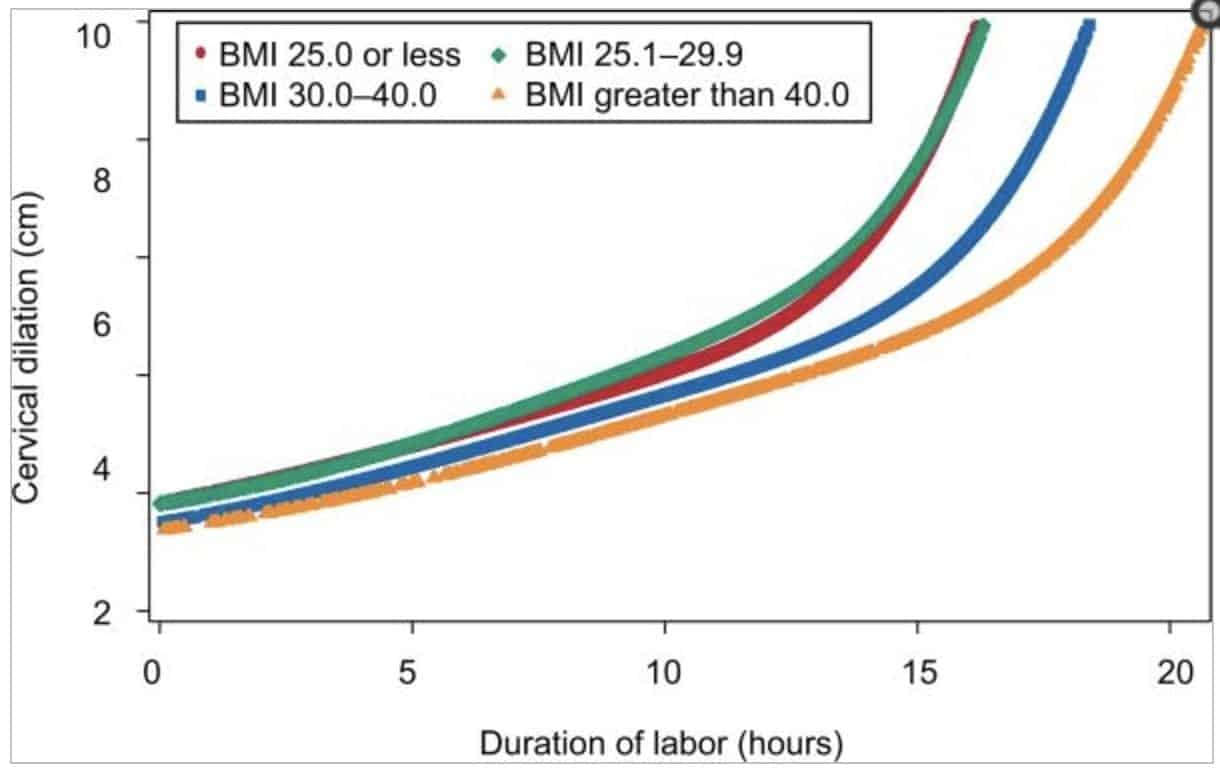
The Friedman curve of labor progression is commonly used to define what is normal and what is abnormal for labour duration. This curve does not take into account individual differences or other contributing factors that can lead to longer labour. As a result, interventions may be used unnecessarily and lead to an increase in cesareans for ‘failure to progress’.
Plus size women are not represented on this curve and norms for management of labour for women with ≥ 30 BMI have not yet been established. Obesity should be considered in defining norms for management of labor (16).
The bias that women with a BMI of ≥30 will fail to progress during their labour leads to the increased risk of interventions such as augmentation and cesarean which we have mentioned pose greater risk for obese women. In the ACOG ‘Safe Prevention of the Primary Cesarean’ consensus states that to avoid unnecessary cesareans slow but progressive labor in the first stage of labor should not be an indication for cesarean delivery.
The idea of a longer labour can be a scary one, but it is important to know that there are other contributing factors that may lead to longer labours. Choose a supportive and loving birth team, attend prenatal classes that include breathing/comfort techniques and hire a care provider that believes in you and your body.
Choosing care providers and being a care provider:
Who a birthing person chooses to have alongside them during pregnancy and birth is essential in creating a positive experience. Feeling supported and respected while in the care of their midwife or OB is the right of all persons, regardless of size. Leaving an appointment feeling shamed or scared because of size, or being talked to as just a BMI is not ok. It’s never ok!
We recommend asking the important questions early on, like ‘do you support my birth preferences?’ and ‘how does my weight affect your care?’. For more information on how to choose a healthcare provider and what questions to ask, please listen to the podcasts listed below. Use these same questions when adding a size friendly doula to the birth team; doulas are also known to reduce the incidence of interventions and negative outcomes!
When looking into care providers, place of birth is also important. The equipment and the staff must be able to accommodate plus size pregnancy and the unique needs of birthing women who fall into this category. Added weight can make diagnostic testing such as ultrasounds and monitoring such as blood pressure and heart rates less accurate unless accommodations have been made. Be sure the team you have chosen has experience in plus size pregnancy, a woman should feel safe and respected in her place of birth and little details like blood pressure cuffs and gowns that fit are important.
Final thoughts and more information:
Biases against plus size women in medicine are very real and it can leave plus size women doubting their strength and their ability to have the healthy birth they hope for.
Something that struck a cord for us was when Kate said ‘don’t get your hopes up until the baby is on the outside of my body’ holding true to this idea that plus size women are often made to feel like their body is broken. It is not! Plus size is not synonymous with unhealthy and it’s time that we start playing by those rules.
We want the takeaway from this article to be that a plus size body does not equal an unhealthy pregnancy or medicalized birth and if you are in the care of someone who makes you feel unsupported or shamed, you have every right to move on.
Positive birth outcomes are possible and most plus size women will go on to have a healthy pregnancy and birth. Pregnancy is a great time for bodies of every size to make healthful choices and changes that will increase the chances of reaching your birthing goals.
Check out our #bopo circuit for more candid discussions on plus size pregnancy and body positivity:
Healthy Births, Happy Babies: Myths & Truths about Plus Size Pregnancy

Mom & Mind: Supporting “overweight” perinatal mothers

__________________________________
References:
-
Statistics Canada. Adult obesity in Canada: measured height and weight. 2005. Available at: http://www.statcan.gc.ca/pub/82-620-m/2005001/article/ adults-adultes/8060-eng.htm. Accessed January 6, 2010.
-
Martin, K E, et al. “The Influence of Maternal BMI and Gestational Diabetes on Pregnancy Outcome.” Diabetes Research and Clinical Practice., U.S. National Library of Medicine, 23 Feb. 2015,
-
Zhang C, Solomon CG, Manson JE, Hu FB. A prospective study of pregravid physical activity and sedentary behaviors in relation to the risk for gestational diabetes mellitus. Arch Intern Med 2006;166:543–8.
-
Crane JMG, White J, Murphy P, Burrage L, Hutchens D. The effect of gestational weight gain by body mass index on maternal and neonatal outcomes. J Obstet Gynaecol Can 2009;31:28–35.
-
Weiss JL, Malone FD, Emig D, Ball RH, Nyberg DA, Comstock CH, et al. Obesity, obstetric complications and cesarean delivery rate–a population-based screening study. Am.J.Obstet.Gynecol. 2004 Apr;190(4):1091-1097
-
https://evidencebasedbirth.com/evidence-for-induction-or-c-section-for-big-baby/
-
Edwards LE, Hellerstedt WL, Alton IR, Story M, Himes JH. Pregnancy complications and birth outcomes in obese and normal-weight women: effects of gestational weight change. Obstet.Gynecol. 1996 Mar;87(3):389-394.
-
Sacks DA, Chen W. Estimating fetal weight in the management of macrosomia. Obstet Gynecol Survey 2000;55:229–39.
-
Sheiner E, Levy A, Menes TS, Silverberg D, Katz M, Mazor M. Maternal obesity as an independent risk factor for caesarean delivery. Paediatr Perinat Epidemiol 2004;18:196–201.
-
Delpapa EH, Mueller-Heubach E. Pregnancy outcome following ultrasound diagnosis of macrosomia. Obstet Gynecol 1991;78:340–3.
-
Rouse DJ, Owen J, Goldenberg RL, Cliver SP. The effectiveness and costs of elective cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA 1996;276:1480–6.
-
Catalano PM, Ehrenberg HM. The short- and long-term implications of maternal obesity on the mother and her offspring. BJOG 2006 Oct;113(10):1126-1133.
-
Robinson HE, O’Connell CM, Joseph KS, McLeod NL. Maternal outcomes in pregnancies complicated by obesity. Obstet.Gynecol. 2005 Dec;106(6):1357-1364.
-
Doherty DA, Magann EF, Francis J, Morrison JC, Newnham JP. Pre-pregnancy body mass index and pregnancy outcomes. Int.J.Gynaecol.Obstet. 2006 Dec;95(3):242- 247.
-
Vahratian A, Zhang J, Troendle JF, Savitz DA, Siega-Riz AM. Maternal prepregnancy overweight and obesity and the pattern of labor progression in term nulliparous women. Obstet.Gynecol. 2004 Nov;104(5 Pt 1):943-951
-
Norman, Shayna M., et al. “The Effects of Obesity on the First Stage of Labor.” Obstetrics and Gynecology, U.S. National Library of Medicine, 7 July 2015